


Alcohol’s SURPRISING Role in Your Health and Longevity
Alcohol is a macronutrient and a source of toxicity like the other macronutrients. And it's hormetic.

The widespread claims in the nutrition and longevity spaces that there is no safe level of alcohol consumption are total nonsense.
In the study widely claimed to show that there is no safe level of alcohol for the brain, going from zero to one alcohol unit (half a drink per day) was not associated with any harm in females, and was associated with slightly better brain markers in males.
Associations between alcohol consumption and gray and white matter volumes in the UK Biobank

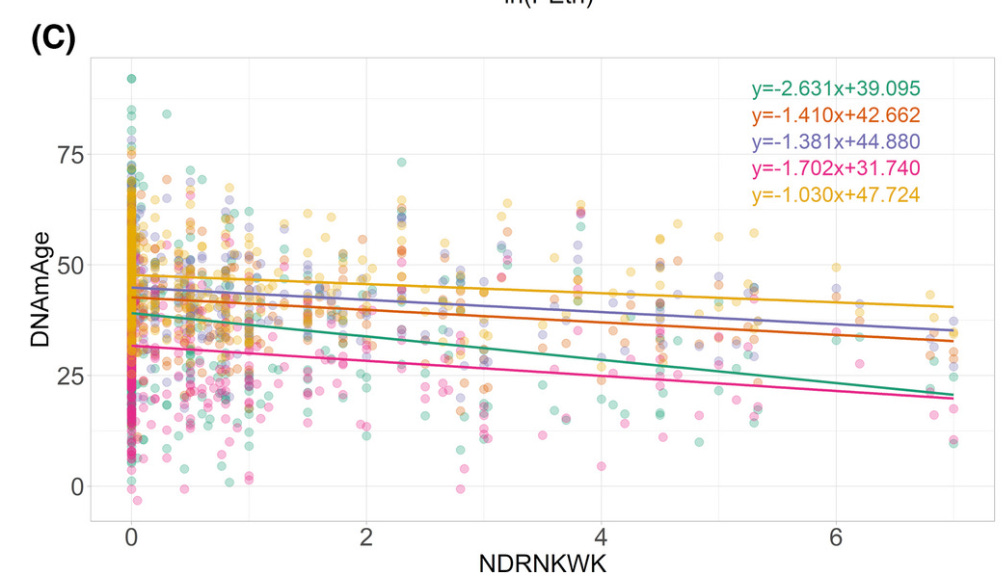
DNA markers of aging go down with increasing number of drinks per week at least through seven drinks per week (one drink per day).
Peter Attia recently claimed that a Mendelian randomization study using genes for “alcohol use disorder” could serve as a proxy for alcohol intake, and that it showed there is no safe level of alcohol for cardiovascular disease.

But alcohol use disorder is not defined simply by the amount of alcohol consumed. It is defined by failing to to meet obligations, being unable to stop drinking, NEEDING to drink in the morning, blacking out frequently, causing physical injury to oneself or others, and behaving in a way that leads others to intervene in your drinking habits.
Calculator: Alcohol consumption screening AUDIT questionnaire in adults (Patient education)
This is not in any way, shape, or form, a proxy for alcohol intake. The authors pointed out that the scores correlate strongly with alcohol intake, but only 16 out of 40 points in the score relate to how much and how often one consumes alcohol.
Consumption of “low” levels of alcohol, meaning up to one drink per day, is associated with a 26 percent lower risk of heart disease and 24% lower risk of all-cause mortality.
Alcohol and Health Outcomes: An Umbrella Review of Meta-Analyses Based on Prospective Cohort Studies

The fact that one drink per day average is associated with lower all-cause mortality is the most important observational finding that can be made, because it accounts for all forms of disease substitution and shows what happens in net.
As can be seen in the figure above, up to one drink per day is also associated with decreased risks of all forms of cardiovascular disease, all but four types of cancer, diabetes, dementia, Alzheimer’s, and chronic kidney disease.
Now, why would this be?
First let’s make it clear that alcohol is not best described as “a toxin.” It can act as a drug and have toxic effects but it is first and foremost a macronutrient.
It is metabolized to acetaldehyde in the cytosol and then to the short-chain fatty acid acetate in the mitochondria, each of which generate usable energy in the form of NADH, then it is converted to acetyl CoA and metabolized the same as acetyl CoA obtained from oxidizing protein, fat, and carbohydrate.
Ethanol is a short-chain fatty alcohol whose metabolism best resembles longer-chain fatty alcohols. These are found naturally in beeswax, whole grains, insects, and a variety of plant foods, in milligram quantities. We also synthesize them endogenously.
Long-chain fatty alcohols use enzymes connected to the endoplasmic reticulum to be oxidized first to long-chain aldehydes and then to long-chain fatty acids, and these then enter the mitochondria using the carnitine shuttle to generate acetyl CoA that enters metabolism as if it had come from anywhere else.
The intermediate, the aldehyde, is toxic. Aldehydes are carbonyl groups (C=O), carbon double-bonded to oxygen. If the carbonyl is in the middle of the molecule, the molecule is a ketone. If it’s on the edge, it’s an aldehyde.
Carbonyl groups are highly reactive, and when they are on the edge of the molecule there is less stuff that can get in between them and whatever they would damage. Smaller molecules fit between things easier and can make the most damage. Thus, small aldehydes are particularly toxic.
However, methylglyoxal is more toxic than acetaldehyde. It’s three carbons rather than two, but it has two carbonyl groups rather than one. Thus it has double the power to damage. Methylglyoxal is derived in small amounts from carbohydrate, protein, and fat.
The accumulation of acetaldehyde will depend on genetics, niacin status, respiratory chain function, and is likely minimized by consuming protein and carbohydrate with alcohol, which will help support the downstream entry of acetyl CoA in to the citric acid cycle.
Acetaldehyde is found naturally in fruits and vegetables, and in fact vegetables have more than wine, and cider has more than vodka.
Even teetotalers have been found to have 430 nanomoles per liter acetaldehyde, compared to 770 nanomoles per liter in alcoholics reporting for treatment.
Methylglyoxal levels are on the order of 200 nanomoles per liter, which is only mildly smaller than the difference between alcoholics and teetotalers for acetaldehyde
Dicarbonyl stress in clinical obesity
Thus, while drinking alcohol certainly poses the risk of compounding total aldehyde toxicity, it isn’t unique in this respect when compared to the other macronutrients.
Further, once alcohol is metabolized to acetyl CoA, it cannot support its own entry into the citric acid cycle without fat or carbohydrate, and in this way it greatly resembles the burning of fatty acids. This is why ethanol is ketogenic.
This is *part* of the reason why “alcoholic ketoacidosis” exists.
Alcoholic Ketoacidosis: Etiologies, Evaluation, and Management
Alcohol’s toxic burden is not exclusively mediated through acetaldehyde. It is also the case that it upregulates CYP2E1 to make acetaldehyde, and CYP2E1 generates reactive oxygen species in the process.
However, this also resembles ketones, because insulin suppresses CYP2E1, and acetone, derived from the major ketone bodies, increases it. CYP2E1 converts acetone in a two-step process to acetol and then to methylglyoxal, which is more toxic than acetaldehyde.
All toxins have the potential to carry out hormetic effects, where a low dose of something bad does something good by improving the fitness response.
For a lesson on the basics of hormesis, see here:
8. Beneficial Toxins: Phytochemicals, Hormesis, and Nrf2

If you’re having issues with playing the video above, play this instead: Hormesis is the principle that a little bit of something bad is good for us because of how we respond to it. The "phytochemicals" in plant foods offer the perfect example of this principle. Here's how it works.
Notably, two primary mechanisms for alcohol would be 1) upregulation of the enzymes needed for alcohol metabolism, which will also increase vitamin A activation since these pathways share enzymes, and 2) low levels of reactive oxygen species are very well established to improve defenses against reactive oxygen species.
Alcohol seems to have a hormetic effect on testosterone in rats.

My suspicion is this is from improved activation of vitamin A, which is involved in upregulating sex hormone synthesis.
It has this effect on the activity of superoxide dismutase, an antioxidant enzyme needed to defend against oxidative stress, in isolated cells.

So, it is very plausible and in fact almost certain that small amounts of alcohol can have beneficial hormetic effects.
The question is, at what dose?
We saw above that up to one drink per day is associated with a lower risk of all-cause mortality, lower risk of the major killers, and improvements in DNA markers of aging, and that a half a drink a day is safe for the brain and possibly beneficial.
Let’s look at some more data:
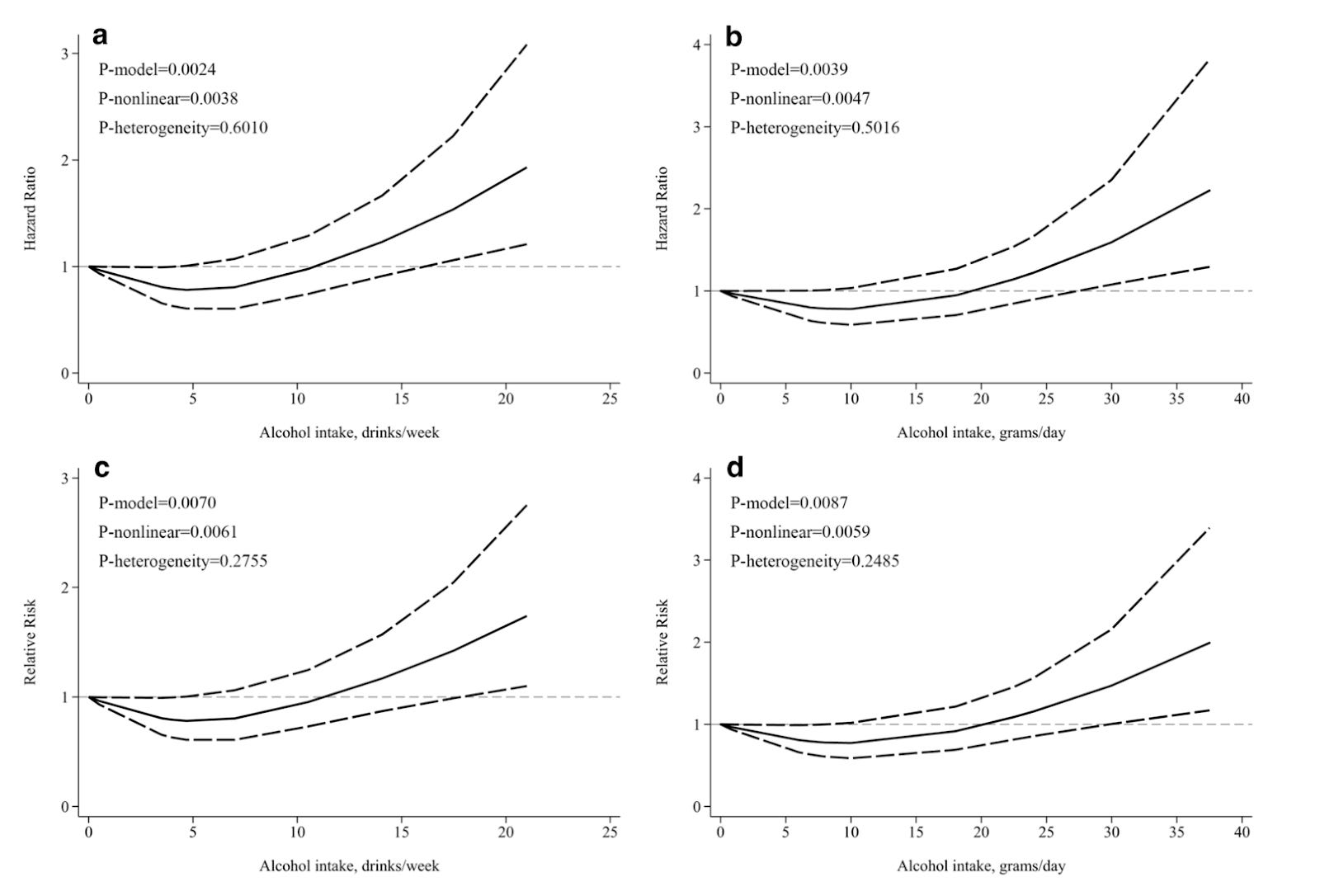
Alcohol at any level seems to be associated with at least a slight increase in the risk of total fracture, but osteoporotic fracture bottoms out at one drink per day. This makes me think any alcohol increases the risk of accidents while a hormetic benefit mediates protection against osteoporosis. That said, the lower bound of the confidence interval does not rise above zero for total fractures until after one drink per day.
Glioma bottoms out around 1-2 drinks per day:
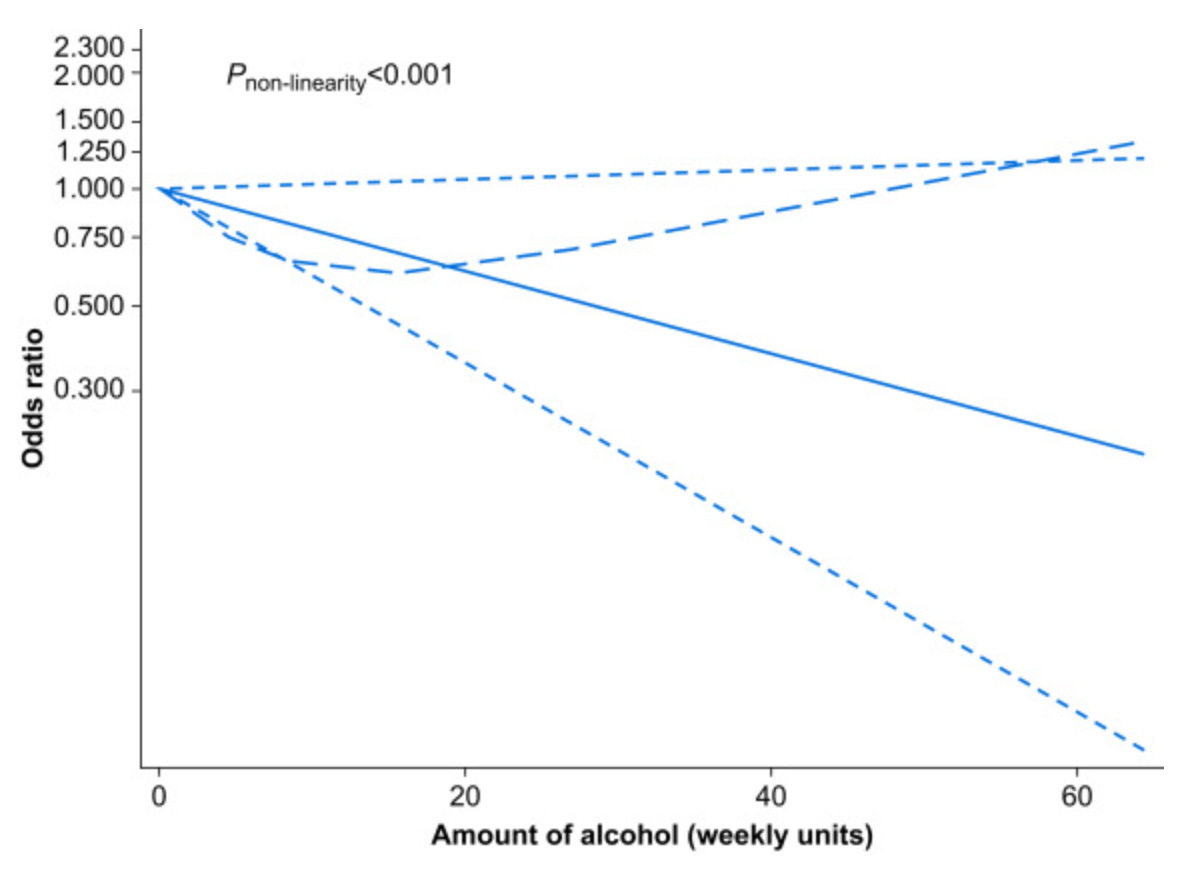
Chronic pain (long dashed line) bottoms out around 1 drink per day

:
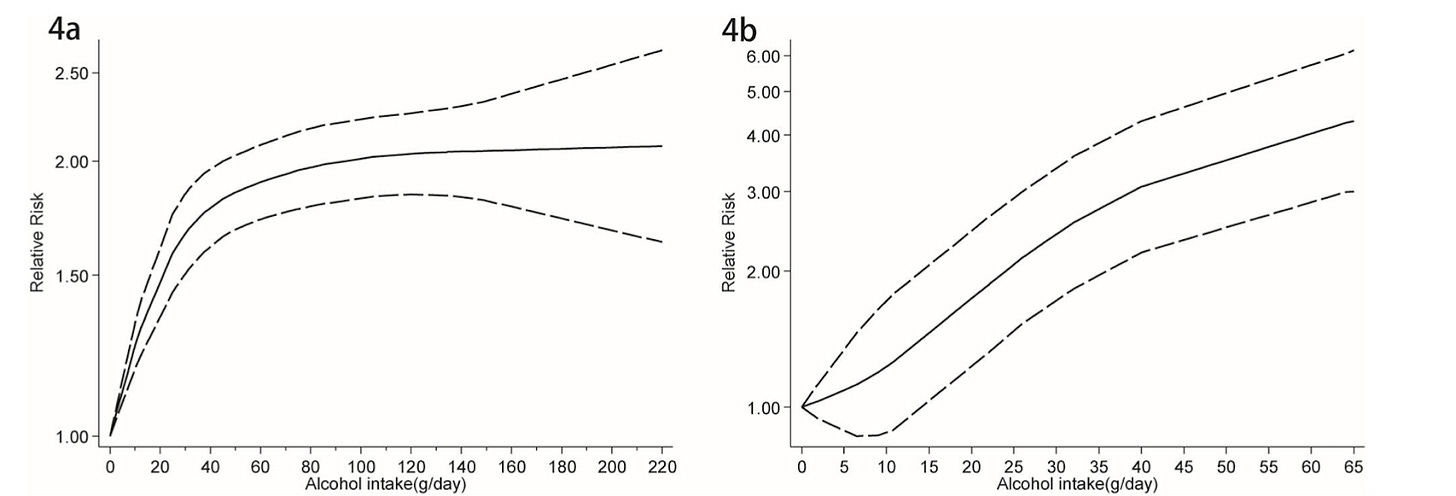
Atrial fibrillation doesn’t really go anywhere until you get to 3 drinks per day, and then takes off upwards.
Risk of Alzheimer’s is lower in any-drinkers than non-drinkers and doesn’t start rising till above two drinks per day.
Parkinson’s bottoms out around two drinks per day:

Bladder cancer risk seems to rise at nearly any alcohol intake.
For kidney disease it looks like the only UNsafe amount of alcohol is zero:

The same is true for kidney stones

Even among Asians, who have an increased risk of acetaldehyde accumulation, diabetes risk bottoms out at one drink per day:

The same is for diabetes more broadly:
Prostate cancer also bottoms out around a drink a day, though the association is weak:

Progression from mild cognitive impairment to dementia bottoms out around one drink per day:

Esophageal cancer has a “no safe amount of alcohol” distribution, though squamous cell carcinoma doesn’t really take off until a half a drink per day:
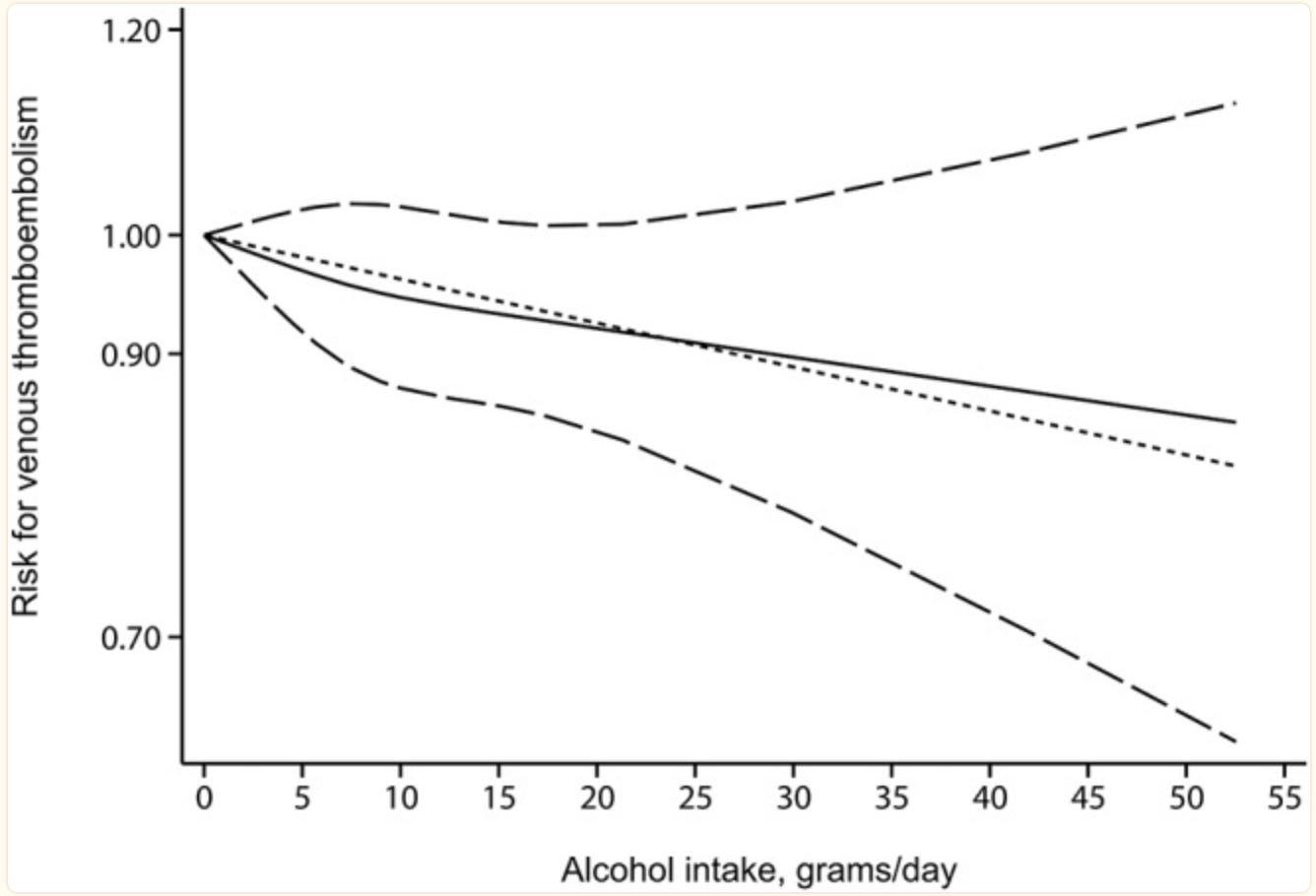
For venous thromboembolism, the only UNsafe amount of alcohol is zero:

Breast cancer risk seems to go up at any dose of alcohol.
Depression bottoms out at 0.7 drinks per day:

For erectile dysfunction, up to 3 drinks a day is associated with lower risk.
For risk of community-acquired pneumonia, there may be no safe level of alcohol consumption.
Nonmelanoma skin cancer follows a “no safe amount” distribution, though the effect size is weak:

For endometrial cancer, the only UNsafe level of alcohol is zero:

For thyroid cancer, the only UNsafe amount of alcohol is zero

No safe level for squamous cell carcinoma, but the effect size is weak.
H. pylori bottoms out at one drink per day:

Liver cirrhosis has a “no safe amount” distribution, but the effect doesn’t really take off until you hit a few drinks a day.
Heart attacks bottom out around 2 drinks per day:

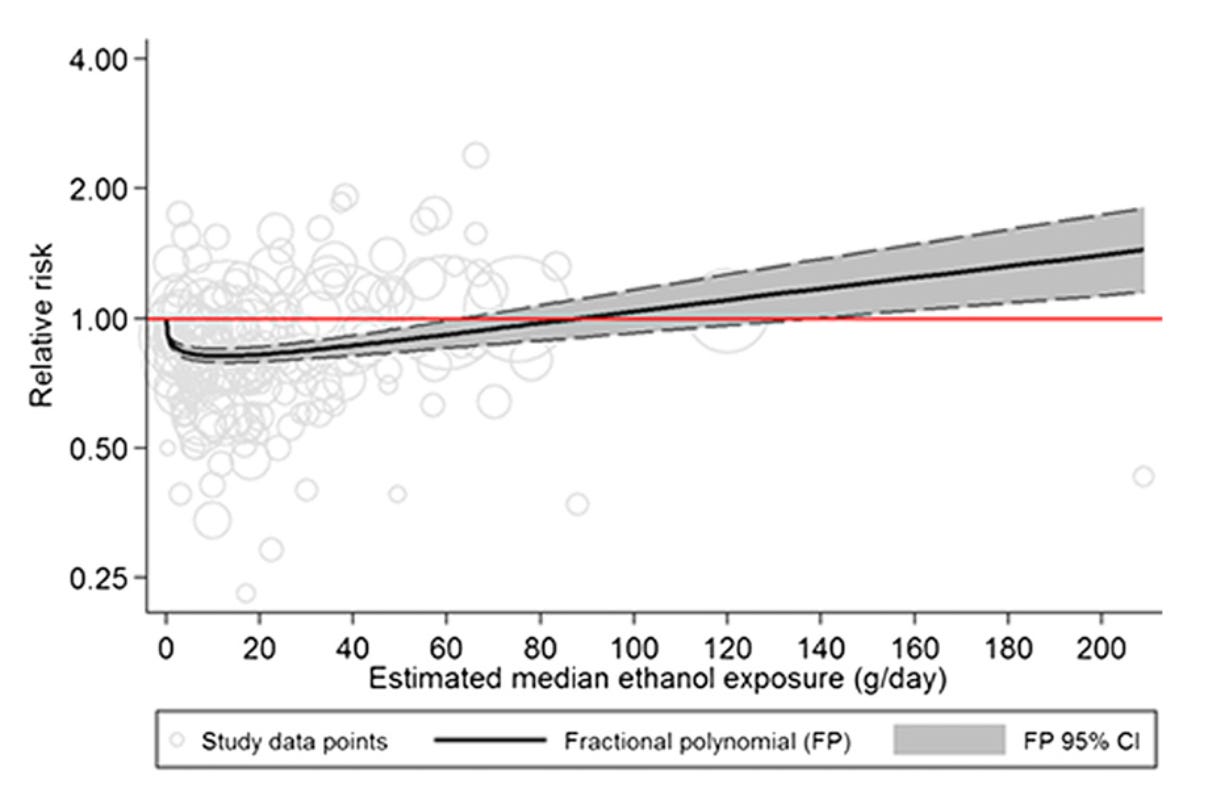
Finally, total mortality bottoms out around 0.3 drinks per day, but stays bottomed out until at least the half a drink per day (7 grams) level:















In conclusion, the optimal dose of alcohol from the totality of the data appears to be in the range of 0.3-0.5 drinks per day, where the risk of total mortality bottoms out.
While there appears to be “no safe amount” for esophageal cancer, community-acquired pneumonia, nonmelanoma skin cancer, breast cancer, squamous cell carcinoma, and liver cirrhosis, the opposite “no unsafe amount except zero” is found for chronic kidney disease, kidney stones, venous thromboembolism, endometrial cancer, and thyroid cancer.
Diabetes, glioma, chronic pain, Alzheimer’s, Parkinson’s, dementia, and H. pylori bottom out around 1 drink per day. Cardiovascular disease bottoms out around 2 drinks per day. Erectile dysfunction stays lowered at up to 3 drinks per day. Depression bottoms out at 0.7 drinks per day.
While these are observational studies and can’t demonstrate cause and effect, cell and animal experiments provide reason to believe alcohol has hormetic effects at low doses mediated by improved activation of vitamin A and increased defense against reactive oxygen species.
A half a drink per day appears to be the average person’s optimal average, given the vast wealth of observational data suggesting total mortality and most disease risks are bottomed out here, and suggesting it is safe for brain volume and beneficial for dementia.
Now this does not mean that everyone’s safe amount is at this threshold. Indeed, alcoholics may be much better off teetotalers, and many people may have higher or lower tolerance.
Since NAD+ is needed for alcohol clearance, not only niacin status but hundreds of mitochondrial disorders could play a role in alcohol tolerance, beyond the well established variation in acetaldehyde dehydrogenase genes.
Moreover, normal food does not simply generate methylglyoxal, a toxin that rivals acetaldehyde, but there are hundreds of metabolic impairments that can generate neurotoxins and cardiotoxins from dietary protein or fat.
For example, if you cannot break lysine down effectively, you will accumulate glutaric acid, a demyelinating neurotoxin, when you eat protein.
I estimate that each person has one to six highly nutritionally actionable genetic mutations that affect whether they metabolize food energy correctly and influence the generation of toxins from food. For more on that, see “How I Found My Health “Super Unlock” After 20 Years of Research and 20,000 Genes Tested.”
In the meantime, don’t drink if you are an alcoholic, and otherwise adjust your alcohol consumption to what makes you feel best, with 0.3-0.5 drinks per day (10-15 per month on average) being the starting point for what is most likely to be beneficial.
From there, listen to your own body.
Join the Masterpass
Masterpass members get access to premium content (preview the premium posts here), all my ebook for free (see the collection of 10 ebook guides here), quarterly question contests (see here), and all my courses for free (see the collection here). Upgrade your subscription to include Masterpass membership with this button:
Learn more about the Masterpass here.
Please Show this Post Some Love
Check Out My Affiliates
At no extra cost to you, please consider buying products from one of my popular affiliates using these links: Paleovalley, Magic Spoon breakfast cereal, LMNT, Seeking Health, Ancestral Supplements, MASA chips. Find more affiliates here.
Very interesting! I had an uncle in Greece who was in his 90's who had a tiny amount of Tsipouro (kinda like grappa) every morning and he was never sick. He accredited his good health to having the tiny amount of alcohol daily. He would always say "ligo!" meaning "a little!" when talking about having the Tsipouro (which was also likely moonshine).
This makes total sense! As a biochemist myself, I’ve often wondered if there was a hormetic effect to a little bevvy now and again...especially given the low levels of consumption across blue zones. My body seems to want to stop after about half a drink these days - maybe this is why!
I’d be curious the effect of ethanol on female hormones, given the huge role the liver plays in their metabolism...and how this may change later in life. (my peri/menopausal female clients always say, “at 45, I stopped being able to drink at all!”)
Once again, thank you Chris 🙏🏻🙏🏻🙏🏻 for your incredible expertise, excellent writing, and for digging up all this fascinating data for us!