


Maybe THIS Is Why You're Hangry
No, I'm not talking about low blood sugar.

If you feel anxious, tense, irritable, more painful, distractible, jittery, more easily startled, or like you’re flat-out going to have a seizure when you haven’t eaten, this doesn’t mean your blood sugar is low.
Maybe it is.
Did you measure it?
If not, then you don’t know it was low. End of story.
I know for myself, I have never been hypoglycemic when I “feel hypoglycemic.” I discovered this by measuring my glucose during those times.
Certainly low blood sugar can cause all those problems, and it can happen when you haven’t eaten.
But here’s another explanation.
As I covered in Will Longevity Diets Wreck Your Hormones?, CoQ10 Deficiency Is Sulfur Toxicity, and The Three Nutrients You Need More Of on a High-Protein Diet, S-sulfocysteine is an excitotoxin that activates NMDA receptors and can cause a spectrum of overstimulation symptoms ranging from irritability to seizures.
Elevated urinary S-sulfocysteine is a hallmark of genetic disorders in the molybdenum-dependent sulfite oxidase enzyme and in the collection of genetic disorders that cause sulfite oxidase deficiency secondary to a deficiency in one of the enzymes that “activate” molybdenum to its cofactor form.
But guess who else has S-sulfocysteine in their urine?
Practically EVERYONE.
Here are the levels in the urine of healthy children (left), the urine of healthy adults (middle), and the blood of healthy adults (right):

A few observations:
One of the 45 children appears to have zero S-sulfocysteine in their urine.
One of the 24 adults with serum samples appears to have zero in their serum, but the lowest urine sample in the 75 adults is just above zero.
The highest adult urine sample is 51 times higher than the lowest adult urine sample, and the spread between those is continuous.
You would think something that is present in everyone’s urine and varies 50-fold that happens to activate NMDA receptors and cause neurological degeneration could be a powerful explanation for a major part of the variability in trait anxiety, muscle tension, ease of being startled, and the risk of neurological and psychiatric disorders.
In patients with molybdenum cofactor deficiency, the levels are on average 27-fold higher:
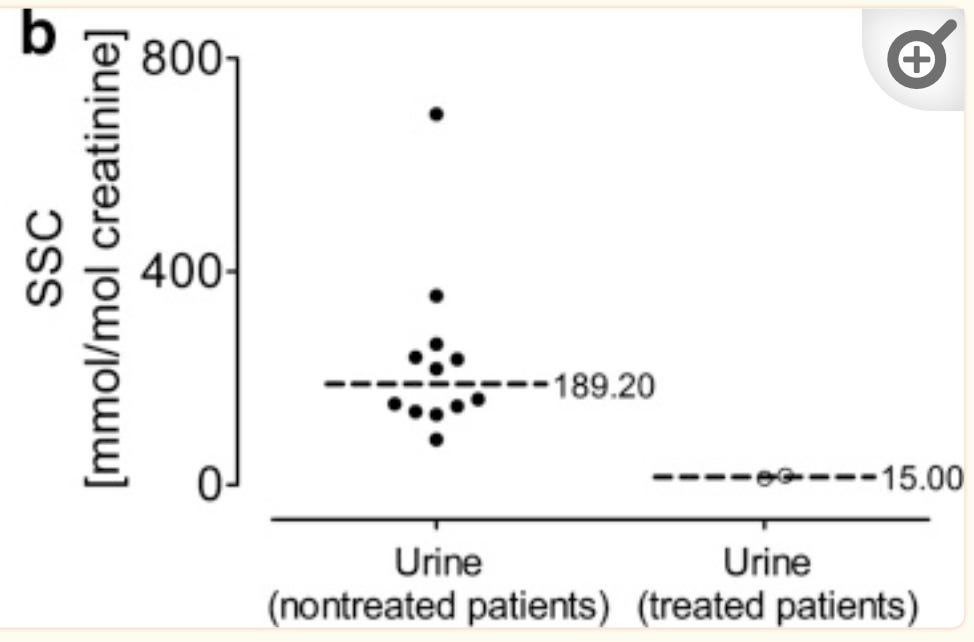
The lowest value is 79, and the highest sample in healthy adults is 25, so they don’t overlap.
But that 27-fold difference in averages is smaller than the 51-fold difference among healthy people.
Two patients shown on the right were treated with a compound that skips over the broken step in their molybdenum cofactor synthesis pathway, and their levels declined to 2.4 times higher than the average in healthy adults. Yet, to a level that was below that found in many of the healthy adults.
To put this another way, S-sulfocysteine excretion is on a continuous spectrum from near-zero to almost 800, and the genetic disorders represent outliers, but I bet you would find a lot more outliers in the supposedly healthy adults if you had a bigger sample size.
The incidence of molybdenum cofactor deficiency as a full-blown genetic disease is between one in 100,000 and one in 200,000, and this outnumbers isolated sulfite oxidase deficiency by about 3:1.
In order to match 14 molybdenum cofactor patients proportionally, they would have needed 1.4-2.8 million ostensibly healthy adults, not 75.
Thus, it is probably the case that there is a “long tail” of “so-called healthy” S-sulfocysteine levels that run between 30 and 79, creating a continuous right-skewed distribution, where variability in anxiety-related psychological traits is explained in the more common zone between 0 and 10, and the risk of neurological and psychiatric diseases increases slowly as you go from the fatter part of the right tail in the 10-20 range and then exponentially as you slide down the long tail on the way from 20 to 800.
Now why could this make you hangry?
As I covered in my previous articles, when you are hungry for glucose, you will break down many amino acids including cysteine to make it. When you make glucose from cysteine, you activate the sulfur catabolism pathways that generate sulfite as an intermediate. If you lack sufficient sulfite oxidase activity to convert it to sulfate, you make more S-sulfocysteine.
Thus, I propose that many people get hangry because they are generating S-sulfocysteine as collateral damage during protein catabolism.
If everyone has S-sulfocysteine in their urine, either it is a normal subsidiary neurotransmitter that acts as an assistant to glutamate in the way that taurine acts as an assistant to glycine and GABA, or most people have dysregulated sulfur metabolism due to crappy nutrition and a variety of idiosyncratic genetic bottlenecks.
It doesn’t really matter which one of these is true. If you’re making more of a neurostimulant than you need because you are hungry for glucose and breaking down protein to get it, then you could be overstimulated in all kinds of ways as a result.
Unfortunately, the siloing off of the fields of inborn errors of metabolism from the fields of normal medicine has irrationally banished S-sulfocysteine into obscurity. The only way to get it tested that I have found so far is the Mayo Clinic’s panel for diagnosing molybdenum cofactor deficiency, isolated sulfite oxidase deficiency, and hereditary xanthinuria.
This should, instead, be on every urinary amino acids panel, and, I would argue, on a standard urinalysis. It should be routinely measured in research on psychological traits and the risk of neurological and psychiatric diseases.
And, it just might be why you’re hangry.
The Sulfur Protocol
Click below to get my Sulfur Protocol:
This reminds me of Andrew Cutler's idea about low-level mercury toxicity causing sensitivity to foods with high levels of unbound thiol compounds, which are all also foods high in sulfur (but not all foods high in sulfur are also high-thiol). Recommend remedies include avoiding those foods, eating a high-protein diet, and molybdenum supplementation.
Fascinating - thank you!