

Testosterone in males supports lean body mass, mitochondrial function, all aspects of sexual function, calm and confident performance under pressure, and general well being.
Testosterone declines with aging, as does lean body mass and mitochondrial function. Most likely, testosterone is anti-aging.
The widespread belief that testosterone drives “male pattern baldness” is likely a fundamental misunderstanding driven by the fact that — as I covered in Handling Creatine Side Effects — the more potent 5-alpha-dihydrotestosterone (DHT) shifts energy into defending the brain and penis and away from defending the hair and ovaries. In men, this means that energy scarcity will cause hair loss instead of loss of sexual and cognitive function. The ideal solution would be to resolve energy scarcity. Since testosterone supports mitochondrial function, intervening at the level of blocking its most potent form to save the hair is likely very unwise. And even though hair loss occurs during aging, such a strategy should not be confused with promoting longevity when it is sacrificing the potency of testosterone.
This article is for men, and for women who are looking for information that will help men. While many of the strategies identified here may help women bring up abnormally low testosterone, and may overlap considerably with strategies to raise estrogen and progesterone, those issues need their own discussion, and the inverse of the strategies identified here should in no way be assumed to help lower testosterone in women with polycystic ovarian syndrome (PCOS) or other situations involving abnormally high androgen levels.
Some types of cancers in both men and women can be promoted by sex hormones. Sex hormone-sensitive cancers are a special topic that are not considered in this article.
This article assumes we want testosterone to go up in the men who will use these action strategies.
Some of the most simple strategies, like losing body fat, can become complicated. For example, low-carb diets are excellent for losing weight, and high-protein diets are excellent for body composition, yet studies show that low-carb, high-protein diets cut testosterone by an average of 33%. How can we resolve this?
This article cuts into the data needed to resolve issues like this and comes up with clear action strategies to sustainably increase testosterone in men.
In This Article:
The Short Answer
The Big Picture
1. Avoid These Ten Nutrient Deficiencies
2. Optimize Your Body Composition
How to Lose Fat Mass Without Losing Lean Mass
Who Are the Underweight Men With Low Testosterone and Low Fertility?
3. Manage Your Macros With an Eye on Sulfur Metabolism
4. Love Your mTOR, Doubt Your Longevity Guru
5. Try One of These Four Herbs
Bonus: Intermittent Hypoxia
Why Exercise Didn’t Make the Cut
This is educational in nature and not medical or dietetic advice. See terms for additional and more complete disclaimers.
This article is likely to be truncated by your email and is best read on the web site using the share button:
The Short Answer
Avoid deficiencies of all vitamins and minerals, but especially of vitamins A and D, iron, B1, B2, B3, magnesium, zinc, sodium, and chloride. Try 2-10 grams of salt as long as it does not cause headache or swelling or raise blood pressure. Resources that will help: the Comprehensive Nutritional Screening, How to Track Your Diet With Cronometer, and the Cheat Sheet.
If overweight, lose weight relying on exercise (six hours per week of resistance training as the main base, with the rest being high-intensity work) to create the caloric deficit. Get down to as low as 12% body fat but reverse course if this lowers testosterone.
If you need to restrict carbohydrate, favor fat over protein; but if you need to keep protein high, make sure you optimize your sulfur metabolism. Resource to help: My Sulfur Protocol.
Avoid rapamycin and metformin for longevity, but metformin may be beneficial if it is treating diabetes. Get your limiting amino acids. If you have high blood pressure or erectile dysfunction, this may mean 5 grams of arginine will help. If you are an athlete, using alkalinizing techniques to preserve glutamine or supplementing 20-45 grams of glutamine per day may help. 2 grams of trimethylglycine (TMG) per day can work by supporting methylation, but methylation is complex and requires 26 nutrients. Resources to help: Comprehensive Nutritional Screening, Interpreting the Genova Methylation Panel, My MTHFR Protocol.
100-400 milligrams per day of tongkat ali has the best evidence for an herb. Other herbs that may help include daily doses of 200-250 milligrams of ashwaghanda, 500-600 milligrams of fenugreek, or 500 milligrams of forskolin.
Use of an altitude tent or a simulated altitude mask for three bouts of 10 hours per week can boost testosterone for those willing to go the extra mile.
The Big Picture
Your brain decides how much testosterone you should make based on the calculation of nutritional abundance, minus energy needed to defend against external and internal emergencies, with a multiplier that adjusts the level up or down according to the life stage you are in.
The primary signal of nutritional abundance is leptin, and the secondary signal of nutritional abundance is insulin.
The primary signal of external emergencies is cortisol.
The primary signal of internal emergencies is inflammation.
Body fat and food intake are the main influences on leptin and insulin signaling. We need to have enough body fat and eat enough food. However, after a certain point, adipose tissue needs to be restructured to accommodate additional fat, and this is considered an internal emergency that elicits inflammation. Further, body fat produces the enzyme aromatase, which converts testosterone to estrogen. Therefore, managing body fat and food intake is a crucial balancing act.
Overlaid on this, there are many nutrients required to make testosterone, and poor nutrient handling can lead to the accumulation of toxins that tank testosterone.
Testosterone is bound in the serum by sex hormone-binding globulin (SHBG), and it is thought that the fraction that is not bound, that is, the free testosterone, is the true measure of what is bioavailable. However, total testosterone should probably not be ignored, because it represents the reserve of what can become free when needed.
Ultimately, what you care about are the effects of testosterone, and these can be influenced by other factors, such as androgen receptor sensitivity. Therefore, you should always use factors such as general well being, motivation, focus, calm confidence under pressure, night-time erections, and libido to track your progress, not just testosterone levels.
With that said, we now move on to the five action strategies.
1. Avoid These Ten Nutrient Deficiencies
Testosterone synthesis is most dependent on vitamins A and D, iron, B1, B2, B3, magnesium, zinc, sodium, and chloride.
Steroidogenic factor-1 is a major molecule that cranks up the expression of many genes involved in steroid hormone synthesis, and it is activated by vitamin A. Vitamin A-deficient rats develop testicular atrophy, and this is associated with low activity of steroid-producing enzymes. In testicular cells, vitamin A can both stimulate testosterone production directly and also antagonize the stimulative effect of luteinizing hormone, indicating the possibility that both too little or too much vitamin A could be a problem depending on which effect wins out.
Synthesis of steroid hormones requires three types of enzymes, two of which depend on iron.
In boys, the combination of vitamin A and iron is just as effective at inducing puberty as androgen replacement therapy.
This study selected boys with “constitutional delay of growth and puberty,” which is the most common cause of short stature and delayed puberty. It is first evident as delayed growth in the first three years of life, and later evident as a failure to go through puberty at a normal time. The results suggest that this problem is due to deficiencies of vitamins A and iron as a result of their role in testosterone synthesis.
The study used 6000 IU of vitamin A per week and 12 milligrams of iron per day. This indicates that the amount of vitamin A required for testosterone synthesis is rather small, about 857 IU per day. However, if you do not convert plant carotenoids to retinol effectively and you otherwise do not eat animal products, it would require four eggs per day to hit this retinol intake. So it is far from meaningless.
Vitamin D is required to incorporate iron into steroid-producing enzymes correctly. A meta-analysis of randomized controlled trials found that vitamin D supplementation increased testosterone, but also increased sex-hormone binding globulin (SHBG) and therefore had no effect on free testosterone. Observational data suggests total and free testosterone are maximized at 30 ng/mL 25(OH)D, and the most robust finding is that men with 25(OH)D above 20 ng/mL have higher testosterone levels than men with 25(OH)D less than that.
As with vitamin A, the story with vitamin D is that you want to avoid a deficiency, not that you want to megadose it as a magic bullet to increase testosterone.
The enzymes that synthesize testosterone also depend on thiamin (B1), riboflavin (B2), niacin (B3), glucose, magnesium and zinc, and are increased by sodium and chloride (salt).
Despite the importance of glucose, we will cover evidence below that replacing carbs with fat increases testosterone.
As covered in my long-form zinc podcast, zinc deficiency leads to low testosterone. On the other hand, in the context of folate supplementation for improved sperm characteristics in sub-fertile men, randomized trials show no effect of adding zinc supplements on testosterone. Thus, once again the evidence favors avoiding deficiency rather than megadosing a magic bullet.
Little else exists on these other nutrients in the randomized controlled trial literature. It nevertheless has to be the case that if a given nutrient is needed for testosterone synthesis, there must be some level of deficiency at which testosterone levels are compromised, and therefore deficiencies of all of these nutrients should be avoided.
These vitamins and minerals are not necessarily the be-all end-all of micronutrient effects.
For example, a non-randomized, before-and-after study in eight healthy males showed that testosterone increased acutely after 10 milligrams of boron and chronically after seven days. Two more rigorous randomized studies in bodybuilders using 2.5 milligrams (here and here) suggested no effect. The difference could be related to the dose, but the long-term safety of 10 milligrams of boron is unclear. The difference could also be related to the study design, since non-randomized studies are less rigorous. The essentiality of boron is controversial, and the mechanism by which it would raise testosterone is unknown. If it is of benefit, it is probably beneficial to people on carnivore diets since it occurs mainly in the cell walls of plants.
The MK-4 form of vitamin K2 has been shown to has been to shown to increase testosterone in rats.
As we will consider in the mTOR section, methylation is important to testosterone synthesis and that depends on 26 nutrients.
Salt — sodium chloride — is the one nutrient that is difficult to uncover a deficiency of with testing, especially since serum levels are tightly regulated and because it isn’t a traditional cofactor for the enzymes but indirectly increases their activity, so it is hard to know what level of salt intake drives optimal enzyme activity.
Salt is 40% sodium, and five grams of sodium is the threshold at which the average person starts experiencing adverse effects, such as headache or swelling. That is 12.5 grams of salt per day.
However, many people may experience an increase in blood pressure with much lower levels of salt than this.
The current official recommendation for sodium is to limit it to 2,300 milligrams to reduce the risk of chronic disease, which means limiting total salt to 5.7 grams per day (including that occurring in natural foods).
The old official recommendation for potassium was 4.7 grams per day based on a study showing that this amount of potassium completely abolished the rise in blood pressure that otherwise occurred in response to salt in salt-sensitive hypertensives. One or two grams of salt is likely to be the minimal effective dose to do anything physiologically.
Action Items
Run the comprehensive nutritional screening:
Include the hair trace mineral analysis add-on for boron status.
Analyze your nutrient intake with Cronometer:
Use the Cheat Sheet to remedy any nutrient deficiencies that are found, especially those of vitamins A and D, iron, B1, B2, B3, magnesium, zinc, sodium, and chloride:
Experiment with gram or multi-gram doses of salt, but cut back or balance with potassium if you experience any rise in blood pressure, headache, or swelling; titrate up slowly and use well being, motivation, focus, calm confidence under pressure, night-time erections, and libido as guides prior to retesting testosterone.
2. Optimize Your Body Composition
In the National Health and Nutrition Examination Survey (NHANES), lower body fat percentages were associated with higher testosterone levels in men, but not in women:

Each dot represents a sample, with women being spread flat on the bottom and men huddling around the red line. The trend seems to be consistent down to the lowest body fat sample, which is 11.4%.
This figure shows the data smoothed out with the red line representing the average and the blue lines representing the 95% confidence interval:

The point where the blue lines are hugging flush to the red line represents the area where the data is very strong, and that starts at 17% body fat and higher. The data become especially sparse around 12.7% body fat and lower.
Indeed, if you go back to the first figure and look at the individual dots, there are plenty of people at 12% body fat who have lower testosterone than people at 25% body fat.
Ideologues of “leaner is better” who do not appreciate biochemical individuality may assume this is all a result of confounding from the many other factors that influence testosterone.
However, once you accept biochemical individuality you have to see this as part confounding from other variables and part the fact that everyone has an optimal body fat percentage that is unique to them. This is the point at which the confidence the brain perceives from having adequate fat storage outweighs the adrenal stress the brain may feel from worrying about nutritional adequacy and the inflammatory stress the body may feel from having to restructure adipose tissue to accommodate the demands of fat storage.
Thinking about it this way, some people with 12% body fat have lower testosterone because they have 12% body fat because for them this leads to inadequate signaling of leptin, the main physiological communicator of adequate total energy stores.
A recent meta-analysis of weight loss trials developed this figure to estimate the gain of total and free testosterone based on age, baseline body mass index (BMI), and the amount of weight lost.

To summarize the general trend, you will gain more testosterone if you start out more obese and if you lose more weight; if you are young, you gain more free testosterone; if you are older you gain more total testosterone.
To estimate how much testosterone you could gain by moving from one BMI to the other, print this out, use B and E if you are under 40 or use C and F if you are over 40, and draw a line from your current BMI to your target BMI using a ruler. Then draw a horizontal line at the point where your diagonal meets the center line, and use the absolute increase on the left or the percentage increase on the right.
For example, using A for the total testosterone increase for all ages pooled together, going from a BMI of 35 to a BMI of 20 is predicted to increase total testosterone by 70% or by 6.5 nanomoles per liter.
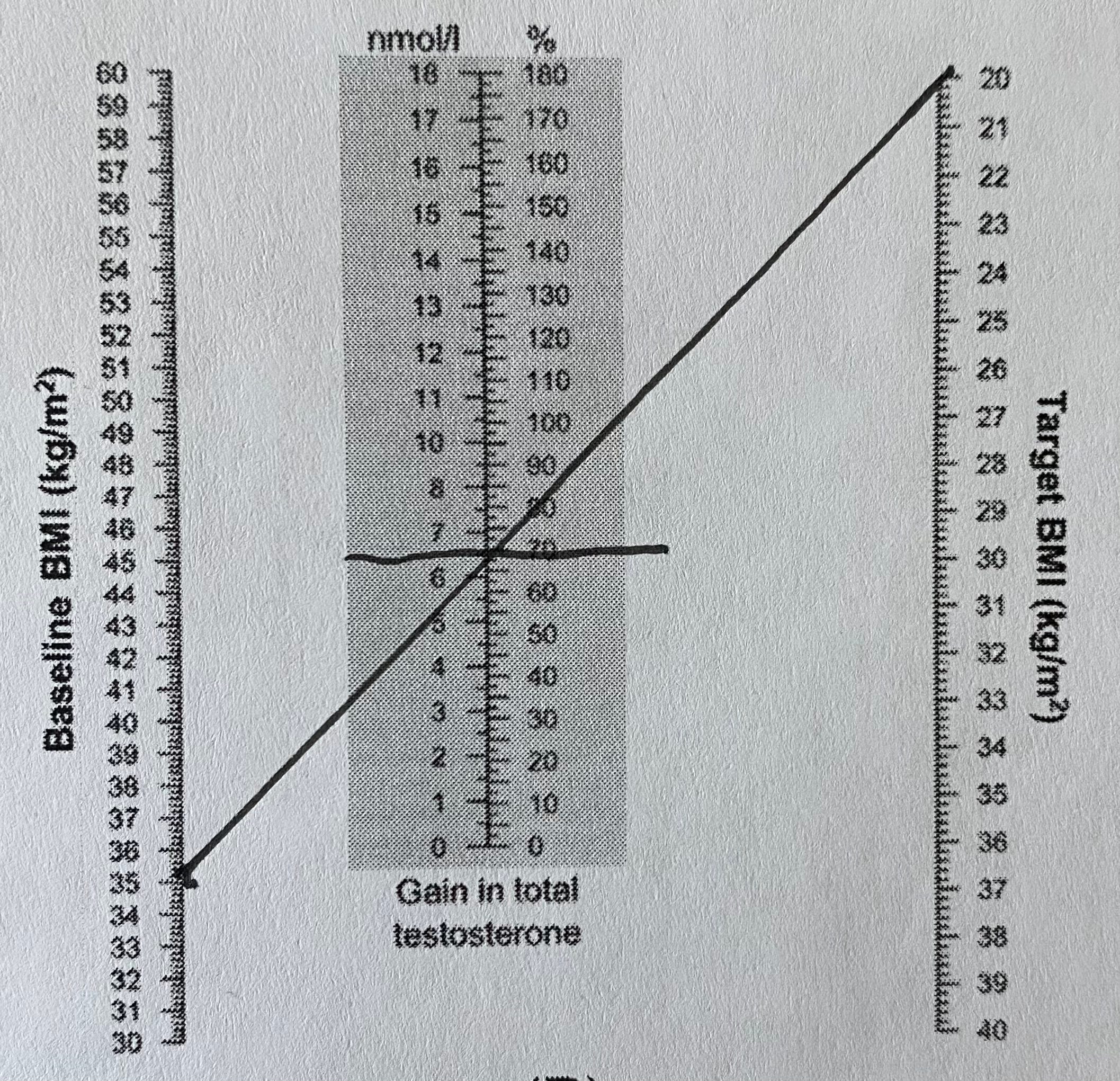
Overall the greatest predicted rise in total testosterone is 220% when a man over 40 goes from a BMI of 60 to a BMI of 20, and the greatest rise of free testosterone is 62% when a man under 40 does the same.
This is clearly an effect of fat loss and not loss of weight (BMI), which is especially clear since the NHANEs study cited above showed that lean mass is positively correlated with testosterone:

The causation in the NHANES results for both body fat and lean mass are likely bidirectional. Testosterone obviously causes increased lean mass, which is why bodybuilders use anabolic steroids. Less widely appreciated, testosterone supplementation leads to fat loss.
However, you cannot do a clinical trial of weight loss that reliably and predictably causes loss of body fat without loss of weight or loss of weight without loss of fat mass. The chart posted above was taken from 44 trials with 1,774 participants. Even this would ideally have a much larger dataset, but the only reason we have a dataset this large is because the less precise but more convenient metric of BMI was used instead of using fat loss.
How to Lose Fat Mass Without Losing Lean Mass
This section has been updated and moved to its own article:
Who Are the Underweight Men With Low Testosterone and Low Fertility?
The fact that there is no such thing as too little body fat for men in the NHANES data is hard to square with other data showing harms of being underweight.
Underweight men have lower fertility than men of normal weight. When couples are considered together both partners being underweight reduces fertility by 10%; when underweight men are paired with obese women, fertility drops by 30%. When the status of the female is held constant, underweight men have consistently stronger reductions in fertility than overweight or obese men.
In people who are not already paired, this is compounded by the fact that underweight and overweight people are less likely to be married, but this is probably driven by perceived attractiveness rather than physiology.
In NHANES, waist circumference is negatively associated with testosterone, except in underweight individuals, where it is positively associated with testosterone. Since underweight status is based on BMI, which in turn is based on weight, and since waist circumference is more reflective of body fat than body weight is, this suggests that there is some degree of insufficient body fat that compromises testosterone synthesis.
Caloric restriction increases testosterone in obese men and decreases testosterone in men of healthy weight.
I believe the best way to synthesize this data is as follows:
The underweight man with low testosterone and low fertility has low fat mass and low lean mass because he doesn’t eat enough food.
If we pair this with the data discussed above for how to lose fat mass without losing lean mass, this all suggests that restricting food intake is a horrible first resort for losing fat mass. Rather, caloric deficits should be established with exercise, because exercise is the most potent way to retain lean mass. After you have achieved two days of full-body resistance training, two days of sprints, and two days of high-intensity interval training or some such equivalent, you can start cutting calories. If you do cut calories you should increase your protein.
I believe this is explained as follows: basal leptin signaling is driven by fat mass; postprandial increases in leptin are driven by insulin; if you have low fat mass and low food intake your leptin declines below that needed to keep testosterone levels high.
There is almost certainly a level at which body fat itself is too low to sustain testosterone synthesis, but this is not what we see in the typical underweight person. Rather, we see that in certain types of elite athletes.
This is hard to capture even in male bodybuilders. For example, those using anabolic steroids have the anabolic steroid use confounding testosterone measurements. Nattys during contest prep get their body fat down from 10.5% to 6.6% while their calorie intake goes from 3000 Cal to 2700-2800 Cal, and this tanks their testosterone by 38%. However, we cannot tease out the low body fat from the caloric restriction.
Thus, if you are below 11.4% you should certainly consider the possibility that raising body fat could improve testosterone, and due to biochemical individuality anyone who finds testosterone going down during fat loss should consider reversing course, but most men should simply focus on losing fat while retaining lean mass.
Action Items
If you are overweight, engage in a weight loss program until your body mass index is at least as low as 25 and continue until your body fat percentage is as low as 12%.
Your caloric deficit should be established primarily by increasing your exercise, not by cutting your food intake. A reasonable target is six hours of exercise per week consisting of resistance training as the primary base, with the remainder based on high-intensity work, including a lot of additional moderate and low intensity exercise for general health. If you keep your protein to at least 1.2 grams per kilogram ideal body weight (0.55 grams per pound), this is sufficient.
If you know of a dietary strategy that works for you to create easy weight loss, use it. For example, some people do better on low-carb, some low-fat, some calorie counting. Use what you know works for you.
If you keep your caloric deficit primarily through exercise as described above, keep weight loss to one pound per week.
If you are unable or unwilling to get your exercise to that level, keep your weight loss to one pound every three or four weeks.
If a low rate of weight loss is discouraging and makes the weight loss program unsustainable, speed it up, but utilize exercise to the fullest extent possible and get protein up to 2.4 grams per kilogram of ideal bodyweight (1.1 grams per pound).
If you find your testosterone dropping as body fat goes below 17% or especially 12%, consider reversing course to see if testosterone goes back up. Everyone has a different ideal body fat percentage and yours might be higher than the average person’s.
3. Manage Your Macros With an Eye on Sulfur Metabolism
The main endocrine regulator of testosterone synthesis in males is luteinizing hormone (LH). LH acts on the testes by increasing cyclic adenosine monophosphate (cAMP). Insulin lowers cAMP, while glucose deprivation increases the production of glucose-regulated protein 78 (GRP78), which enhances the testosterone-boosting activity of cAMP. Thus, carbohydrate and insulin signaling oppose testosterone synthesis at the cellular level.
On the other hand, carbohydrate also stimulates insulin, which increases leptin. Leptin increases thyroid hormone, which mobilizes cholesterol uptake for general downstream utilization, including the conversion of cholesterol to testosterone. Insulin also acts on the thyroid alongside TSH, to produce thyroid hormone. Leptin acts on the hypothalamus indirectly to increase testosterone synthesis, and directly increases pituitary release of luteinizing hormone. Genetic leptin deficiency in men is associated with lack of puberty and low total and free testosterone. Leptin treatment has induced puberty in a 27-year-old leptin-deficient man. Thus, carbohydrate and insulin signaling favor testosterone synthesis at the physiological level.
On a single-meal level, the evidence is clear that eating suppresses testosterone, suggesting that the suppression of cAMP and GRP78 overrides the acute increase in leptin after a meal.
Testosterone is highest in the fasting state, and decreases by 15% after a mixed meal. In saliva, it decreases 18% after an oral glucose tolerance test. It even declines 22% after a meal that is 86% fat and 11% carbohydrate, but this high-fat meal still doubles postprandial insulin despite the low carbohydrate intake.
On the other hand, over the long-term, carbohydrate intake seems to support testosterone synthesis.
A recent meta-analysis found that low-carbohydrate diets lower testosterone; however, when separated by protein intake, only diets that provide more than 35% of calories as protein lower testosterone. Such diets cut testosterone by over one-third. Low-carbohydrate diets that had more fat and less protein were associated with 9% lower testosterone, but this was not statistically significant.
The conclusion from this is that fat is only slightly less supportive of testosterone synthesis than carbohydrate, while protein tends to suppress testosterone.
This doesn’t make any sense when explained in the context of exposure to glucose and insulin. Protein stimulates insulin more effectively than fat, and protein can form glucose far more effectively than fat, making protein naturally aligned with carbohydrate in this respect. Yet the studies just cited place protein as the odd man out in suppressing testosterone.
Further, adding protein to the basal diet does not suppress testosterone. Whey protein supplementation has no effect on testosterone in healthy young men over one day or 12 weeks, and two weeks of it leads to higher testosterone post-training than soy protein despite it being higher in sulfur amino acids. This indicates that extra sulfur amino acids from dietary protein do not suppress testosterone in the absence of carbohydrate restriction.
I believe the explanation is as follows:
As I covered in The Three Nutrients You Need More Of on a High-Protein Diet, high protein diets raise the need for biotin, B6, and molybdenum. Without molybdenum, high intakes of sulfur amino acids lead to accumulation of sulfite. As I covered in The Unknown Testosterone Nutrient, sulfite decreases testosterone. The niacin used in testosterone synthesis is primarily in the form of NADPH. As I covered in How Sulfite Destroys Your Mental Health, sulfite depletes NADPH. As I covered in Will Longevity Diets Wreck Your Hormones?, carbohydrate restriction increases the breakdown of sulfur amino acids.
It may be the case, then, that the effects of macros are largely driven by sulfur metabolism when sulfur metabolism is not optimized. When it is optimized, the effects of cAMP, GRP78, and leptin duke it out, with cAMP and GRP78 usually winning over leptin as they do in the acute postprandial period, implying that low carbohydrate diets could raise testosterone given the right opportunity to do so.
Action Items
If you have a reason to restrict carbohydrate, focus on fat instead of protein.
If you have a goal related to body composition or athletics that involves eating a higher-protein diet in the presence of carbohydrate restriction, try optimizing molybdenum status using the Cheat Sheet to preserve or perhaps even increase testosterone levels.
If molybdenum fails to work for this purpose, engage in a more comprehensive approach to trouble-shooting with the Sulfur Protocol.
4. Love Your mTOR, Doubt Your Longevity Guru
The mammalian target of rapamycin, mTOR — appropriately named after a pharmaceutical since pharmaceutical companies created biology, along with the world and everything therein — increases testosterone synthesis.
The mechanism is as follows. The first step in synthesizing testosterone is brining cholesterol into the mitochondrion so it can be converted to pregnenolone. This is accomplished by steroidogenic acute regulatory protein (StAR), which activates in response to luteinizing hormone. Various intermediate regulators cause StAR to be opposed by cortisol and metformin but increased by the mammalian target of rapamycin (mTOR)
Longevity Drugs Hurt Testosterone
mTOR inhibitors (rapamycin and hydroxethyl-rapamycin) lower testosterone when used in transplant recipients. This is supported by four observational studies that are cross-sectional or case-control in nature, and vaguely supported by one randomized controlled trial that compared a minor difference in the dose between groups and found that the high dose led to non-significantly lower testosterone than the low dose. In one case report, a man became infertile on rapamycin and this resolved by switching to tacrolimus, an immunosuppressant that acts on a different mechanism that does not involve mTOR.
In animals, monkeys are more vulnerable to fertility effects of rapamycin than rodents. For example, rapamycin causes testicular atrophy in rats at one to three times the dose given to humans, but does the same in monkeys at 0.4-1.0 times the dose given to humans.
The doses of rapamycin that extend lifespan in mice destroy their healthspan: they cause glucose intolerance, fatty liver, heart fibrosis, and testicular atrophy. Using intermittent dosing instead of chronic dosing gets rid of the glucose intolerance. However, both males and females develop fatty liver, and the males develop heart fibrosis and testicular atrophy.
Using the lengthening of lifespan in mice to place a bet on this drug extending lifespan in humans is crazy because those same studies show that it obliterates healthspan.
In any case, blocking mTOR lowers testosterone in humans according to the data available.
Metformin in theory could do the same. However, metformin is usually given to diabetics, and it could lower exposure of the testes to glucose and insulin, which could improve testosterone synthesis. In 106 obese men, 850 milligrams of metformin twice a day seemed to result in slightly less total testosterone at six months that normalized after one year, and very slightly less free testosterone, but neither of these were statistically significant.
The question remains what metformin does to testosterone when given to healthy people who do not need it to control blood glucose but are looking to leverage it for longevity. My guess is it would decrease testosterone.
mTOR Nutrients Boost Testosterone
Nutritionally, mTOR is a sensor of nutrient supply. It response to meals that generate a lot of insulin (driven especially by calories and carbohydrate) and to the amino acids arginine, leucine, asparagine, glutamine, and the methionine derivative and universal methyl donor S-adenosylmethionine.
We covered effects of caloric restriction and carbohydrate restriction above.
Studies suggest five grams of L-arginine will boost testosterone:
In 108 diabetic males with mild to moderate erectile dysfunction with a mean age of 43, 5 grams of L-arginine for eight weeks increased testosterone by 46%, from 11.04 nmol/L to 16.19 nmol/L
In 120 males over the age of 60 with erectile dysfunction, 5 grams of L-arginine for six weeks increased testosterone by 19%, from 11.43 nmol/L to 13.7 nmol/L.
On the other hand, in active cyclists and triathletes four weeks of arginine aspartate providing 5.7 grams of arginine and 8.7 grams of aspartate had no effect on testosterone. Similarly, a cocktail of 6 grams of arginine, 4.4 grams of ornithine, and 24 milligrams of B12 for three weeks had no effect in young male weight lifters and bodybuilders.
One frustrating thing about these studies is they do not look at the background intake of protein, arginine, or any other nutrients. It could be that diabetics and older men with erectile dysfunction all have low arginine status driven by inflammatory arginine degradation or low protein intake, whereas the young athletes have less inflammation and consume more protein.
The first two studies showed that tadalafil (Cialis) was just as effective or, in the second study, more effective. Tadalafil blocks the breakdown of cyclic guanosine monophosphate (cGMP), which is made in response to nitric oxide. Nitric oxide is made from arginine. The simplest explanation of this suggests that arginine is boosting testosterone by boosting nitric oxide. The second study showing it to be less effective than the first could reflect other factors dictating nitric oxide production: it depends on zinc and sulfur, it is activated by calcium, it indirectly depends on a variety of other nutrients that are involved in synthesizing and recycling its cofactor, BH4, and it is hurt by oxidative stress. None of this was measured in either study.
Some but not all mechanistic studies indicate that arginine activates mTOR partly through generating nitric oxide, and that this is mediated by cGMP. Nitric oxide promotes testosterone synthesis in rat cells at low concentrations, and hurts testosterone synthesis at high concentrations.
Overall this indicates that arginine will boost testosterone synthesis when its levels are insufficient for normal nitric oxide production. Good indications this could be the case would be high blood pressure and erectile dysfunction; this could be directly tested with a plasma amino acids test.
Two studies indicate glutamine boosts testosterone:
3 weeks of 0.3 grams per kilogram bodyweight per day L-glutamine (45 grams per day for a 150 pound person) increased salivary testosterone by 24% in combat sport athletes.
In boxers, half that dose of glutamine did not have a statistically significant effect on salivary testosterone unless it was combined with alkaline water. The combination had a similar effect as found in the first study. Notably, physical activity generates acidity, which leads to the hydrolysis of glutamine to glutamate to release ammonia to buffer the acidity.
These studies may indicate that athletes blowing through huge amounts of glutamine through high levels of physical activity may benefit from high-dose glutamine in the range of 45 grams per day. They may also benefit from using alkaline water to prevent glutamine depletion, which could cut the dose of glutamine required to boost testosterone in half.
Leucine does not seem to impact testosterone during days or weeks in athletes during intense training periods. This may be because they are already consuming enough leucine from dietary protein.
I cannot find any studies on methionine or asparagine supplementation.
However, betaine, also known as trimethylglycine (TMG), increases the conversion of methionine to S-adenosylmethionine, the form of methionine that activates mTOR. In professional youth soccer players, testosterone went down in the placebo group over a 14-week season and went up in a TMG-supplemented group. At the end of the season, testosterone was twice as high in the players receiving 2 grams of TMG per day, one gram two hours before training and the other one hour after training.
Folate does not seem to increase testosterone, and I cannot find trials with B12.
I explained in Your Cells Are Starving for Creatine why TMG is a much simpler test of the effect of methylation than folate or B12.
Nevertheless, methylation depends more broadly on 26 nutrients, so whatever your limiting nutrient is may raise testosterone in you personally. The Genova Methylation Panel is the best way to assess methylation.
Altering protein intake from 50 to 82 grams does not impact testosterone over a four-day period, but this may be too short of a time period to see the overall effect.
As discussed above, whey protein supplementation has no effect on resting testosterone in healthy young men over one day or 12 weeks, but two weeks of it leads to higher testosterone post-training than soy protein despite it being higher in sulfur amino acids. Notably carbohydrate leads to a similar support of post-training testosterone, and carbohydrate is also important for mTOR activation.
The overall implication of this is that the weakest link in mTOR activation will boost testosterone when the total mTOR stimulation is inadequate. For athletes, this is most likely acidity-induced glutamine degradation. For men with erectile dysfunction, this is most likely arginine-induced nitric oxide production. For the average person, more protein, more carbohydrate, or more calories may be needed to activate mTOR.
Action Items
Avoid rapamycin and metformin if trying to boost testosterone, but keep metformin if it is successfully treating diabetes.
If you have high blood pressure or erectile dysfunction, try five grams of L-arginine.
If you are an athlete, try alkaline water, baking soda, carnosine, or beta-alanine to buffer acidity; 20-45 grams of glutamine may be needed to boost testosterone; more effective buffering of acidity should lower the dose of glutamine required.
Two grams of trimethylglyine (TMG) may increase testosterone over fourteen weeks. If an athlete, try taking one gram two hours before training and one gram one hour after training.
The plasma amino acids test in the Comprehensive Nutritional Screening will help narrow down the limiting amino acids in an individual.
Add the Genova Methylation Panel to determine your personal weak spot in your methylation.
5. Try One of These Four Herbs
A meta-analysis of tongkat ali supports a strong effect on boosting testosterone at doses between 100 and 400 milligrams per day for between three weeks and six months. Effects generally range from 14% to 55% increases, with roughly twice the effect size in hypogonadal men as in healthy men.
Randomized trials of ashwaghanda support 225 mg increasing testosterone by 11%, 240 mg having no effect, 200 mg increasing testosterone 10%, 600 mg having no effect or increasing testosterone 17%.
Randomized trials of fenugreek support 500 mg increasing testosterone by 23%, or increasing free and total testosterone slightly but without statistical significance, and 600 mg having no effect or increasing testosterone by 11%, or having no effect on total testosterone but increasing free testosterone by 11%.
One trial of 500 milligrams of forskolin for twelve weeks raised total testosterone by 44% but free testosterone was only 4% higher.
Overall the strongest data for herbal methods lies with tongkat ali at a dose of 100 to 400 milligrams per day.
Action Item
Try 100-400 milligrams per day of tongkat ali.
If that doesn’t work, 200-250 milligrams of ashwaghanda, 500-600 milligrams of fenugreek, or 500 milligrams of forskolin may have some benefit.
Bonus: Intermittent Hypoxia
Hypoxia activates the same testosterone-boosting mechanism as mTOR.
In rats, eight hours per day of hypoxia for 14 days increases testosterone, but in mice, chronic sustained hypoxia for 12 or more hours decreases testosterone progressively over time.
In boxers, 10-12 hours per day in a hypoxic chamber during evening hours and sleep for 11 days increased testosterone at the 20-hour mark but this increase had started to return toward baseline by day 5. This suggests that everyday use of hypoxia is not optimal even over 11 days and is not sustainable.
In cyclists, the same protocol was applied except that hypoxia was endured three times per week for four weeks. Testosterone increased 31% from 490 to 645 ng/mL, stayed elevated through the entire study, and went back to baseline after the protocol was stopped.
By contrast, in eight heathy young men a single resistance training session under hypoxic conditions had no effect on testosterone compared to the same session in normoxic conditions, and in healthy male college students, twice a week resistance training in hypoxic conditions for five weeks did reduce cortisol but had no effect on testosterone. This indicates that a couple hours per week of hypoxia is insufficient stimulus to raise testosterone.
The intermittent hypoxia training used in boxers and cyclists is called the Live High Train Low routine, and it can be replicated by sleeping in an altitude tent.
Hypothetically, it could be replicated by using a simulated altitude mask for the same number of hours per week.
The best results were obtained from the cycling study where hypoxia was only used on three days per week. Testosterone levels fell back to normal after hypoxia was stopped in the fifth week. Therefore, this should be considered a practice done three times a week to maximize testosterone for durations lasting up to four weeks, and longer use should be checked against its effect on testosterone levels and all other indicators of health and well being.
Personally, I find this the most cumbersome approach, but if you are really trying to optimize for a performance goal, enduring 30 hours a week of moderate hypoxia might be worth it.
Action Items
An altitude tent or a simulated altitude mask used for 10-12 hours three times a week may be used for up to four weeks (possibly longer) to boost testosterone by 31%. To conform to the studied methods most closely, use the tent in the evening and during sleep.
Why Exercise Didn’t Make the Cut
There is robust evidence that exercise transiently increases testosterone for about 30 minutes, with the intensity of the exercise driving the degree of the testosterone boost.
This is, of course, important for the physiological effects of the exercise itself but totally meaningless for boosting overall testosterone unless it translates into a cumulative effect.
Twice a week resistance exercise causes testosterone to rise over 14 weeks and then sink back to baseline by the end of 21 weeks.
There are overall conflicting studies on whether moderate intensity endurance exercise increases or decreases testosterone, while sustained overdoing of high-intensity exercise decreases testosterone.
In sports players, testosterone is generally lower at the end of the season. For example, I cited a study of youth soccer earlier where testosterone declined over the 14-week season and TMG not only rescued it but raised it. In male power athletes, testosterone went up 21% in the first five weeks of a ten-week season and then went down 19% in the second five weeks. The soccer player study indicates that nutritional support is just as important as rest in order to prevent exercise from tanking testosterone.
Overall the message of exercise is to not go to extremes, and to emphasize adequate recovery and nutritional support.
Exercise should be sought out for the benefits to body composition, strength, cardiovascular fitness, balance, stability, and functional movement, and should not be manipulated for a direct effect on testosterone.
However, if you are a couch potato, you will likely increase your testosterone by fixing that.
The Bottom Line
Avoid deficiencies of all vitamins and minerals, but especially of vitamins A and D, iron, B1, B2, B3, magnesium, zinc, sodium, and chloride. Try 2-10 grams of salt as long as it does not cause headache or swelling or raise blood pressure. Resources that will help: the Comprehensive Nutritional Screening, How to Track Your Diet With Cronometer, and the Cheat Sheet.
If overweight, lose weight relying on exercise (six hours per week of resistance training as the main base, with the rest being high-intensity work) to create the caloric deficit. Get down to as low as 12% body fat but reverse course if this lowers testosterone.
If you need to restrict carbohydrate, favor fat over protein; but if you need to keep protein high, make sure you optimize your sulfur metabolism. Resource to help: My Sulfur Protocol.
Avoid rapamycin and metformin for longevity, but metformin may be beneficial if it is treating diabetes. Get your limiting amino acids. If you have high blood pressure or erectile dysfunction, this may mean 5 grams of arginine will help. If you are an athlete, using alkalinizing techniques to preserve glutamine or supplementing 20-45 grams of glutamine per day may help. 2 grams of trimethylglycine (TMG) per day can work by supporting methylation, but methylation is complex and requires 26 nutrients. Resources to help: Comprehensive Nutritional Screening, Interpreting the Genova Methylation Panel, My MTHFR Protocol.
100-400 milligrams per day of tongkat ali has the best evidence of an herb. Other herbs that may help include 200-250 milligrams of ashwaghanda, 500-600 milligrams of fenugreek, or 500 milligrams of forskolin.
Use of an altitude tent or a simulated altitude mask for three bouts of 10 hours per week can boost testosterone for those willing to go the extra mile.
What Has Helped Your Testosterone?
Let me know in the comments!
Have had amazing results with pine pollen tincture along with nettle root powder which were recommended in Stephen Harrod Buhner's book Natural Remedies for Low Testosterone:
How to Enhance Male Sexual Health and Energy.
I have only used the tincture from Woodland Essence he recommended. The nettle root from Swanson in caps.
I use Buteyko breathing to raise carbonate blod levels. See Originally learned of this from Ray Peat but Patrick McKeown's many books have expanded my knowledge greatly. I get overheated in a hurry wearing a respirator when exercising or mowing the lawn (to avoid exhaust fumes.
Thanks for sharing Chris!
When I was a marathoner, I was also vegan and experimenting with a raw food diet. My body fat dropped to 5%. Then the ION Profile showed me that many of my imbalances (esp amino acids) could be corrected by adding animal products to my diet. I also had very low testosterone levels at that time. Now that I’m around 15-20% body fat, my testosterone levels are well into the healthy range. So my experience is consistent with your article.