


The Worst Longevity Idea Ever Conceived
The last thing you want to do is perpetually inhibit your mTOR.

Rapamycin is a darling of the longevity community.
I find it very hard to read the literature on this molecule without shuddering at the idea of taking it to lengthen lifespan.
And yet, it can benefit your mitochondria — but only if you use it very carefully.
I have heard it said that rapamycin is the leading longevity molecule because of the robustness of the literature in mice.
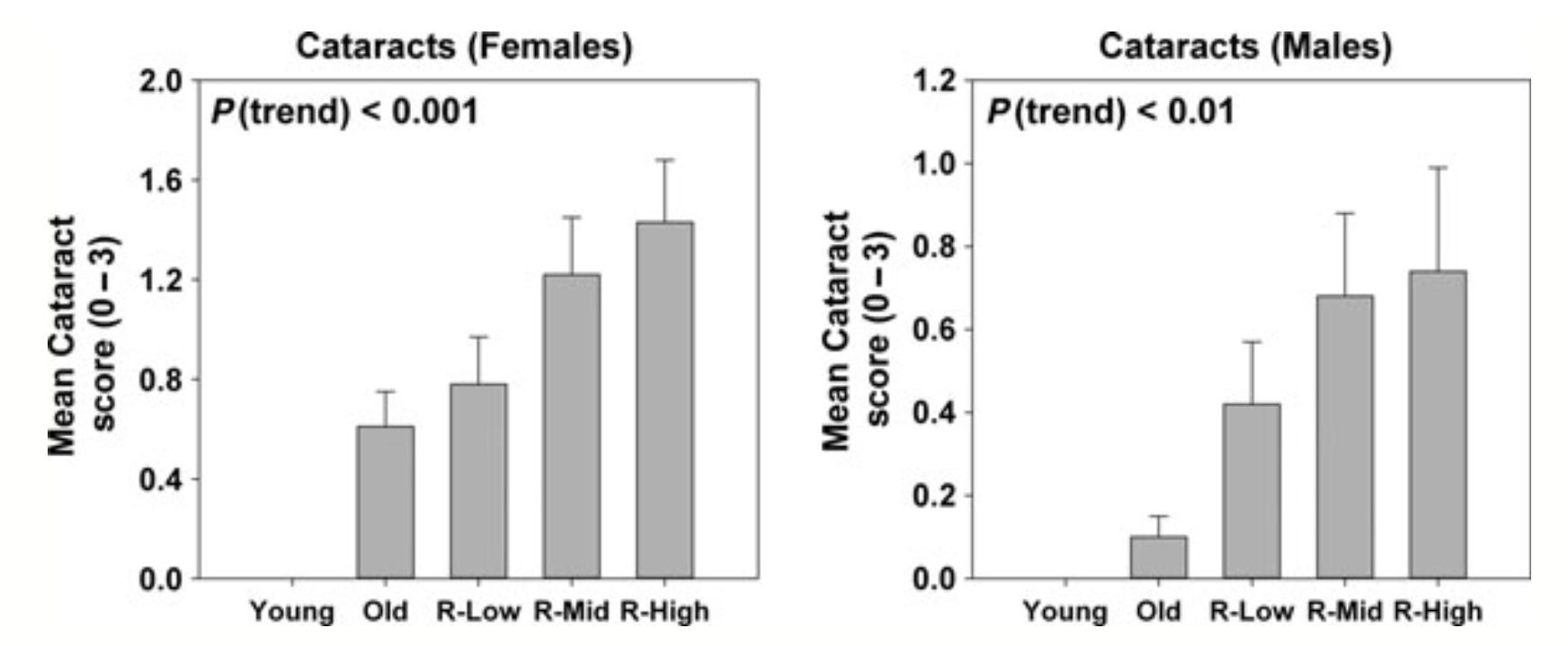
But what the literature in mice robustly shows is that it causes cataracts, testicular atrophy, and impaired glucose metabolism at doses beneath those that lengthen lifespan. When you get into lifespan-lengthening doses, this just gets worse. And other problems are added, like fatty liver and heart scarring.
In other words, rapamycin lengthens lifespan at profound expense to healthspan.
I have also heard it said that if you get canker sores from it, you know it’s working.
If it is drilling a hole in your mouth, what do you think it’s doing to your brain? Rapamycin inhibits the synthesis of lipids and collagen and impairs the healing of wounds. It blocks the synthesis of lipid-rich myelin just the same.
Below I will argue that rapamycin can indeed help turnover damaged mitochondria when used in a temporary series of fasting-feeding cycles, but outside its possible use for genetic defects in breaking down old cellular components, it should not be used in perpetuity.
The basic problem with rapamycin is this:
It inhibits mTOR, a signal of nutrient abundance.
We are meant to cycle through nutrient scarcity and abundance during ordinary fasting-feeding cycles.
When things are scarce, we clean house. When things are abundant, we rebuild. Think of it as selling off all the old clothes in your closet to raise money and make room for new ones. Endlessly cleaning out your closet doesn’t in and of itself get you nice things.
There is no master signal of nutrient abundance. There are, instead, a complex web of nodes that all synergistically signal nutrient abundance. These include, among others, mTOR, leptin, insulin, citrate, ATP, and NADH. You can’t take one molecule to mimic fasting and expect it to work the same as actually fasting. And you certainly can’t expect to take it in place of fasting while eating an abundant diet and expect nothing to go wrong.
Life Extension In Mice Comes At Huge Costs
Rapamycin lengthens lifespan in mice. However, it also scars their hearts, raises their glucose, fattens their liver, and shrinks their testicles.
Dosing the rapamycin intermittently in mice rather than chronically partially but not entirely mitigates the impairment in glucose metabolism. Intermittent dosing extends lifespan just as much as chronic dosing in male mice, but detracts from the lifespan benefit in female mice.
Intermittent dosing of rapamycin does nothing to mitigate the scarring of the heart, the atrophy of testicles, or the fattening of the liver.
Rapamycin inhibits glucose oxidation via the citric acid cycle, which is what you would expect in the fasting state. The impairment in glucose metabolism probably comes from taking a fasting-mimicking compound while the mice are not fasting.
You try to fool the body? The body will fool you.
The intermittent dosing group in this study got the full dose of rapamycin alternated with no rapamycin on a weekly basis.
The dose was 42 milligrams of rapamycin per kilogram diet. This was based on another study showing maximal lifespan extension at this dose. However, that older study used an often-repeated approach of comparing 4.7, 14 , and 42 milligrams per kilogram diet. 42 milligrams every other week is an average of 21 milligrams per kilogram diet. Thus, it may be that males do not need a dose higher than 21 mg/kg diet.
These doses are the bodyweight- and surface area-adjusted equivalent of a 70-kilogram or 154-pound human taking 2, 6.5, or 19 milligrams per day.
Most commonly, those in the anti-aging community are using doses of of 5-7 milligrams once a week, which yields 857 micrograms per day, about 43% of the lowest dose used in mice.
In mice, the median increase in lifespan on the three doses is 3%, 13%, and 23%. The lowest dose has a P value of 0.19 and is not statistically significant.
Thus, the dose commonly used in the anti-aging community is about 43% of the dose that fails to extend lifespan in mice.
While the low dose fails to increase lifespan in mice, even that dose causes a massive increase in testicular degeneration and cataract formation:

The non-life-extending low dose causes just as much glucose intolerance as the moderately life-extending medium dose:

Abolishing the impairment in glucose metabolism requires bringing the dose down from 2 milligrams per kilogram bodyweight per day to the same dose administered once per week:

In this study the rapamycin was injected. 2 milligrams per kilogram bodyweight per day is about 25 milligrams per kilogram food per day, and thus around the maximally life-extending dose. Cutting this to once a week yields the equivalent of 3.6 milligrams per kilogram food, underneath the dose that fails to increase lifespan. Thus, in mice, abolishing the glucose intolerance means abolishing the lifespan benefit.
In this study, the lower dose only decreased T regulatory cells in the spleen by 25% compared to 60% in the higher dose.
A decrease in T regulatory cells would be expected to dysregulate the immune system in favor of autoimmunity, and it occurs even beneath the dose associated with lifespan extension.
3.6 milligrams per kilogram food is the equivalent of a human taking 1.6 milligrams per day or 11.4 milligrams per week.
On the one hand, this suggests that the anti-aging community is operating slightly below where the adverse effects stop in mice.
On the other hand, this is well below the point where significant lifespan extension occurs in mice.
Monkeys Get Worse Arthritis Without Living Longer
Studies in marmosets, a type of monkey, using 1 milligram rapamycin per kilogram bodyweight per day general do not show the metabolic destruction found in mice, but the doses used in the marmoset studies also fail to impact DNA methylation markers of aging and fail to make them live longer. This overall suggests that the rapamycin either does very little in these animals or the doses used are just to low compared to those needed to extend lifespan. However, rapamycin worsened osteoarthritis in both marmosets and mice at similar bodyweight-adjusted doses, emphasizing that adverse health effects start beneath the life-extending doses.
Humans Get Trashed Testosterone, Oral Inflammation, and Impaired Wound Healing
The testicular atrophy that occurs in male mice lines up well with human evidence that rapamycin lowers testosterone when used in transplant recipients. This is supported by four observational studies that are cross-sectional or case-control in nature, and vaguely supported by one randomized controlled trial that compared 3 milligrams per day to 1.5 milligrams per day and found that the high dose led to non-significantly lower testosterone than the low dose. In one case report, a man became infertile on rapamycin and this resolved by switching to tacrolimus, an immunosuppressant that acts on a different mechanism that does not involve mTOR.
1.5 milligrams per day for a human is about 70% of the low mouse dose that fails to extend lifespan.
This suggests that a subtly testosterone-limiting dose in humans may be beneath the lifespan-extending dose.
While the adverse effects in this study may have been confounded by the kidney health of the participants and their experience of surgery, and the other drugs used, adverse effects were experienced by almost everyone, leading to almost 20% discontinuing the medication, including over 21% with urinary tract infections, 1.7-2.9% with pneumonia, 24% with anemia, and 4% with new-onset diabetes.
In subjects with progressive lung disease, 1-2 milligrams of rapamycin per day led to massive rates of side effects in the first month, with a very gradual leveling off over two to three years:
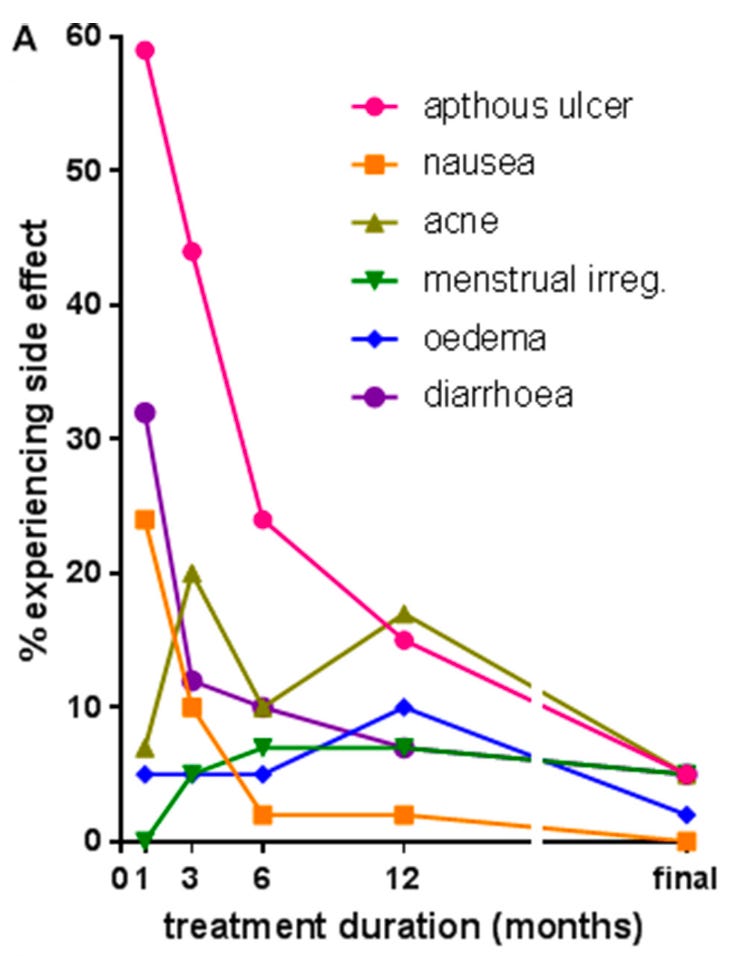

Canker sores (apthous ulcers) occurred in 58% of people to start and were still occurring in 15% by the end of a year. At maximal followup, this had declined to less than 10 percent, but the total rate of inflamed oral mucosa was 13% at the final followup.
Diarrhea started at over 30%, fell to 10% after a year, and disappeared at final followup.
Nausea started out at 24% but was short-lived.
The persistence of canker sores and oral inflammation into final followup is very concerning.
Canker sores like any other ulceration are likely driven by the balance of tissue degradation from acidity and inflammatory enzymes on the one hand, and tissue synthesis on the other.
The occurrence of canker sores probably reflects the general impairment in wound healing that rapamycin causes. Modern literature considers this an outdated concern, because the use of lower exposure levels and modern regimens no long causes surgery complications from impaired wound healing.
However, chronic low-dose rapamycin clearly inhibits the healing of canker sores. This is likely from inhibiting lipid synthesis and collagen synthesis.
If this is what it does to your oral mucosa, what do you think it is doing to your brain?
mTOR is needed for myelin synthesis and blocking mTOR impairs myelin synthesis. Studies do not universally show a benefit or harm of rapamycin to myelin or the nervous system. However, when rapamycin is combined with cuprizone, a copper chelator that induces demyelination, it hurts the healing process and leads to more inflammation and neuronal damage.
There are many animal studies that show neurological benefits of rapamycin. Most likely rapamycin is harmful when the limiting factor to neurological health is the ability to synthesize proteins and lipids needed for remyelination, but it’s ability to stimulate mitochondrial turnover described below is beneficial when the limiting factor is turning over damaged mitochondria.
Rapamycin Does Have Mitochondrial Benefits But Likely Has to Be Used VERY Carefully to Reap Them
Unlike metformin, which inhibits complex I, rapamycin has no effect on specific respiratory chain complexes, and through secondary effects on metabolism it has been shown to alleviate the phenotype of complex I deficiency in fruit flies and mice and to do the same for complex II deficiency in fruit flies, and for CoQ10 deficiency in mice and human cells, and protects against complex V inhibition by the oligomycin toxin in human cartilage cells.
Sacsin is a protein involved in autophagy. Mutations in this protein cause impaired autophagy, as well as impaired mitophagy, a specific type of autophagy required to remove damaged mitochondria. However, in cellular models of sacsin deficiency, extending the time of autophagy using rapamycin can completely restore normal autophagy and mitophagy.
It is likely that the turnover of damaged mitochondria is most relevant when an acute exposure to a toxin — such as the antibiotic ciprofloxacin — or cumulative damage with aging has led to damaged mitochondria that are not being destroyed and replaced efficiently.
Whether rapamycin is required or simply one of the best ways to deal with this probably depends on whether someone has a genetic impairment in autophagy or mitophagy. In such as case, it could be that the maximal stimulus provided by a potent drug is extremely helpful.
On the other hand, it could be that Urolithin A and/or a fasting-feeding reset is a sufficient and overall safer approach.
My suspicion is that rapamycin has utility for use as an accentuator of the fasting phase of a fasting-feeding reset under the following conditions:
It is taken intermittently where it corresponds to an extended “fasting phase” that is, at minimum, very low in carbohydrate and hypocaloric with at least a portion being water fasting, followed by an equally aggressive rapamycin-free refeeding phase.
The half-life measurements might be exaggerated by measurement in unhealthy populations, but the prevailing beliefs about how long it lasts in the body suggests that it should be taken once with at least one week being considered the corresponding fasting phase. I would argue that a buffer of two weeks should be given before starting a refeeding phase. As an example, take 7-8 milligrams once at the beginning of a two-week period where a portion is extended water fasting and the rest is a very low-carb, hypocaloric diet; then institute an aggressive two-week rapamycin-free refeeding period that leads to the full regain of any weight lost in the first phase.
This should not be done in perpetuity. Each cycle should be assessed for empirical benefit. If repeated cycles show diminishing returns, the practice should be stopped. If the benefits begin to wear off over time, you can experiment with another round of cycles.
Only people with verified genetic defects in autophagy and mitophagy should attempt to carry this on indefinitely.
For more extended guidelines on such an approach to a fasting-feeding cycle with other enhancers of each side of the cycle, see my Fasting-Feeding Reset:
Rapamycin: The Verdict on Longevity
Since the mouse studies show that there is no dose of rapamycin that extends lifespan without degrading healthspan, I consider rapamycin to be one of the worst longevity ideas ever conceived.
mTOR is a nutrient sensor. If we want to leverage it toward longevity, it should be with nutrition.
However, as I covered in Does Molybdenum Lengthen Lifespan?, glycine is an mTOR activator, yet lengthens lifespan.
Methionine restriction lengthens lifespan, but so does increasing molybdenum cofactor synthesis.
The intersection of methionine, glycine, and molybdenum cofactor synthesis is all on sulfur. Most likely, minimizing excessive hydrogen sulfide, sulfite, and S-sulfocysteine is the path to longevity that ties these all together, so if I had to make a bet, I would bet on my Sulfur Protocol outperforming rapamycin for boosting both healthspan and lifespan. You can get it here:
To the extent glycine lengthens lifespan beyond its buffering of sulfur catabolism, this argues for using my glycine protocol:
Using glycine to lengthen lifespan and boost healthspan likely requires minimizing its generation of oxalate. And for that, there is my oxalate protocol:
Rapamycin, in my view, should be used only in the limited context above, in a temporary set of fasting-feeding reset cycles.
Much needed article. I have ruminated for a long time based on my reading that, while living with mTOR permanently active leads to modern lifestyle diseases, being permanently under the influence of AMPK is undesirable and equally a mistake, a point well made in Mattson’s paper on neuroplasticity. I’m so glad to see this confirmed in black and white in another great post from you.
Excellent write up. Could you do a deep dive on Spermidine please?