
IgA Antibodies, Vitamin A, and COVID-19
IgA Antibodies, Vitamin A, and COVID-19

There are four types of antibodies that each have different functions: IgM, IgG, IgA, and IgE. Generally IgE are responsible for classical allergy symptoms, while IgA are particularly important for protecting the mucous membranes of the eyes, nose, mouth, and gastrointestinal tract. In the immune response to an infectious disease, IgM usually appear first, followed by IgG and IgA, with occasional contributions from IgE.
Current antibody tests for COVID-19 test only IgM and IgG, and assume that IgM represents a recent infection, while IgG will represent a recent or distant infection.
Consider this test, which uses this graph to describe its principle:
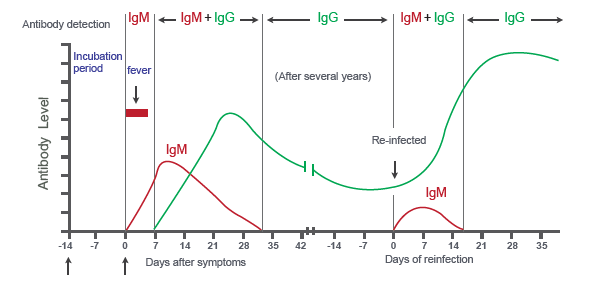
IgM comes first, followed by IgG. IgM disappears rather rapidly, while IgG stays elevated for a very long time. Therefore, IgM suggests recent infection whether IgG is present or not, while IgG alone suggests an infection in the more distant past.
This paper on the first SARS virus provides a more nuanced graph that includes IgA:
It doesn't look as clean as the first graph, but the IgM still comes first and disappears faster than the IgG. The IgA comes last and disappears the fastest.
A preprint* released today by French researchers found things work completely differently in COVID-19:

Unlike the first two graphs, where the antibody level was plotted, in this graph, it is the percent of people with a positive test. On the left are antibodies against the portion of the spike protein that binds to ACE2 to gain entry into the cell, and on the right are antibodies to the protein coating around the virus's genetic material.
In the first week, there are nearly twice as many people who are positive for IgA to the spike protein than those who are positive for either of the other antibodies. IgA continues to be most prevalent in the second week, and it is almost as prevalent as IgG in the third and fourth weeks. IgM is never the most prevalent, and it drops off in the fifth week just like IgA. Only IgG remains prevalent in the fifth week.
The pattern is similar for the antibodies to the protein coating, except IgA only dominates in the first week and has less of a lead on IgG.
IgA antibodies were five times more effective than IgG antibodies at neutralizing SARS-CoV-2, the coronavirus that causes COVID-19.
The patients whose IgA had the greatest ability to neutralize the virus were the ones who had the highest levels of IgA against the spike protein. The spike protein is the graph on the left above, where IgA dominates IgG the most in the early response.
That suggests that during the major period when the virus is being fought off, it is IgA antibodies against the spike protein that offer the most important defense in people who produce them effectively.
This also suggests that the existing antibody tests are based on false assumptions. IgA, rather than IgM, should be used to indicate a recent infection. The authors suggest that we may even be able to use saliva samples to test for IgA against the virus, which would be especially useful for home testing.
If there is a nutritional strategy to leverage to get a better IgA response to the virus, it is probably avoiding vitamin A deficiency. In mice, vitamin A deficiency compromises the production of flu-specific IgA during flu infections. 200,000 IU of vitamin A given at months 3 and 9 of a one-year study (working out to 1095 IU per day) increased IgA levels and decreased respiratory diseases in 6-month-old to 3-year-old children in China. Similar dosing schemes, however, did not impact IgA in the tears of children from northern Ghana, or anti-polio IgA responses to polio vaccines in infants from Zimbabwe.
In The Food and Supplement Guide for the Coronavirus, I recommended avoiding vitamin A deficiency, but also avoiding high-dose supplementation with vitamin A out of concerns that it could raise ACE2 levels. Studies are not unanimous on the effect of vitamin A on IgA levels, but they suggest that IgA is mainly compromised in deficiency, and that even doses below the RDA have positive effects in deficient children.
At the present time, then, it seems that IgA might be one more reason to make sure we are not deficient in vitamin A, but that caution about high-dose supplementation is still warranted.
Stay safe and healthy,
Chris
Please Support This Service
These research updates are made possible by purchases of The Food and Supplement Guide to the Coronavirus. The guide contains my most up-to-date conclusions about what we should be doing for nutritional and herbal support on top of hygiene and social distancing for added protection. Due to the absence of randomized controlled trials testing nutritional or herbal prevention, these are my best guesses for what is likely to work without significant risk of harm, based on the existing science. By purchasing the guide, you are enabling me to continue devoting my skills to the most important issue we now face. I am genuinely grateful for your contribution. You can purchase the guide using this link.
You can get the guide for free if you pre-order my upcoming book, Vitamins and Minerals 101: How to Get the Nutrients You Need on Any Diet (to be released when the COVID-19 crisis subsides) or when you join my membership program, the CMJ Masterpass, which is meant to help people with significant health and wellness expenditures consistently save money by returning marketing cost of the companies involved back to the members as rebates.
For other ways to support my work, please see here.
Disclaimer
I am not a medical doctor and this is not medical advice. I have a PhD in Nutritional Sciences and my expertise is in conducting and interpreting research related to my field. Please consult your physician before doing anything for prevention or treatment of COVID-19, and please seek the help of a physician immediately if you believe you may have COVID-19.
Subscribe
If you aren't subscribed to the research updates, you can sign up here.
Archive
You can access an archive of these updates here.
Comments and Questions
To leave a comment or question, please use the Facebook post for this newsletter.
*Footnotes
* The term “preprint” is often used in these updates. Preprints are studies destined for peer-reviewed journals that have yet to be peer-reviewed. Because COVID-19 is such a rapidly evolving disease and peer-review takes so long, most of the information circulating about the disease comes from preprints.